DIGITAL DENTISTRY-THE FUTURE
Dr. Anumita Deka (P.G Student), Dr. Vinay Mohan (Professor & Head), Dr. Kushdeep Kumar Gupta (P.G Student), Department of Oral Medicine and Radiology, K.D. Dental College and Hospital, Mathura India
ABSTRACT
Digital Dentistry is an emerging technology in dental field, which will enhance patient’s treatment modality in future. It provides digital equipment available to cosmetic dentists and implant dentists. Digital dentistry is not a wave of future, its occurring now. Several digital methods have been incorporated to dental practice to replace conventional methods and techniques in order to enhance treatment planning and predictability of execution. Nowadays, digital dentistry is considered a whole field of study within dentistry. The purpose of this article is to examine the concept of digital dentistry, its advantages and limitations and make statements and observations in specific areas of digital dentistry based on research.
Keywords: Digital dentistry, CAD/CAM, Cone beam computed tomography, Caries diagnosis and Digital workflow in Periodontology.
INTRODUCTION
It’s quite amazing to think about the dentistry performed today as compared to 30 years ago or even 10 years ago. The advances in dentistry state clearly that the dental profession has experienced an exciting amount of technological growth. Yet in comparison to medicine, bio-medical engineering, automotive or aeronautics, electronics and others, dentistry appears to be more than a decade behind in adopting or integrating new technologies on a wide spread basis.1 The success of incorporating a new technology in the office is dependent on the knowledgebase of not only the dentist but the entire dental team. The knowledge of the digital workflow of the different technologies enhances the confidence and the use of these technologies. As with any other field of study, digital dentistry involves a learning curve to be mastered and used in the clinical routine. Ultimately, the dental professional is responsible for using existing digital tools appropriately for patient treatment.2
In the dental world, it means using any digital technology or device involves computer versus mechanical or electrical stand-alone technology or service. This transformed how people communicate, learn or work. The array of digital equipment available to cosmetic dentist, general dentist and implant dentist etc has increased significantly. Such advancements in dental technology enabled patients to receive modern solutions to traditional dental problem.3
The following list represents the majority of areas, which incorporate some type of digital components4
- Shade Matching
- Caries diagnosis
- Occlusion and TMJ analysis and diagnosis
- Computer-aided implant dentistry- including design and fabrication of surgical guides.
- Digital radiography-Intraoral and Extra oral including cone beam computed tomography (CBCT).
- Electrical and surgical implant hand pieces.
- Photography – Extra oral and Intraoral.
- Practice and patient record management – Including digital patient education.
- Lasers.
- CAD/CAM and intraoral imaging – both laboratory and clinician controlled.
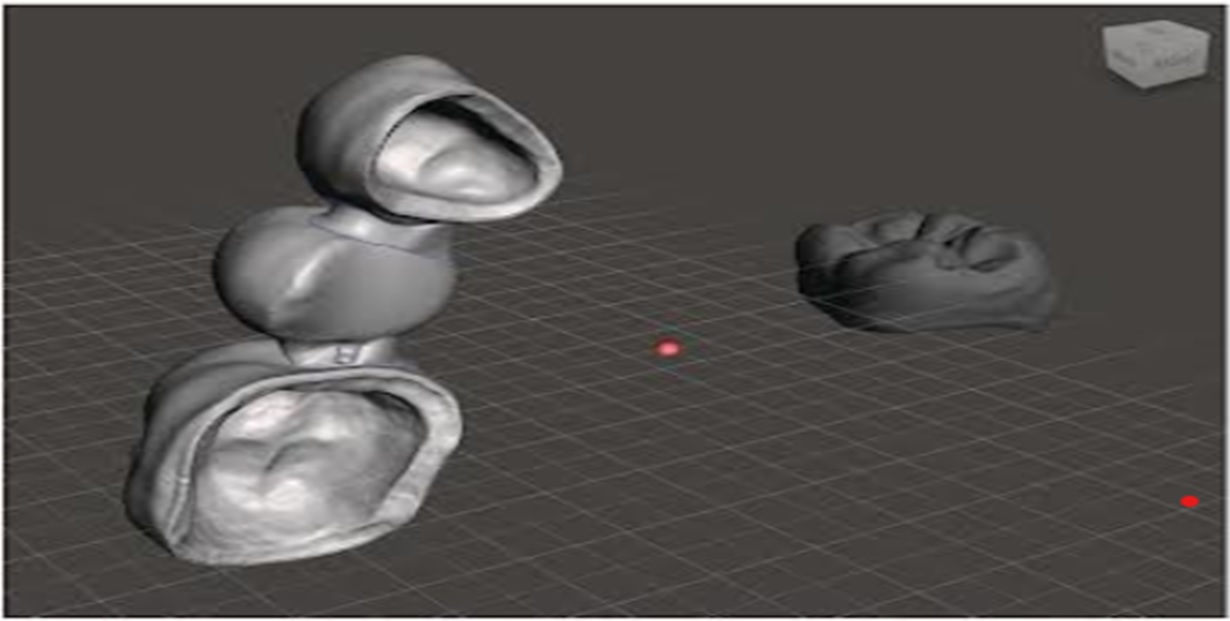
Figure:1.1 Three-dimensional objects imported in different coordinates of the 3D space. Note that the fixed bridge is closer to the screen than the molar crown. The dynamic grid is used to orientate the spatial disposition of the 3D objects.
CAD/CAM
Computer aided design (computer assisted manufacturer) technology enables dental restorations such as crowns, dentures, inlays and onlays to be fabricated using computerized milling technologies. It is faster, more economical, predictable, consistent and relatively accurate. Merging of procedures such as, Implant placement and immediate provisionalization through strategic company alliances and shared technologies allows dentists to do more in less time. CEREC has been available nearly 30 years, and also recent advances with both CEREC as well as E4D clearly demonstrate that the chairside CAD/CAM is uniquely positioned in order to lead our profession in the field of digital dentistry. The future advances in CAD/CAM will better align the dentistry with that most of the other industries are using CAD/CAM for complete predictability of outcomes considering all the extraneous variables. This would include automatic restoration design with no further modifications based on all patient factors such as skeletal and arch classifications wear age, and tooth conditions, excessive movements, TMJ condition, exact inputs of condylar movements in relation to tooth positions, and design based on esthetics and desired looks. This would help dentist to complete tooth restorations on the same day that would otherwise require two or more visits to complete.5.

Figure:1.2 The TRIOS 4 intraoral scanner (3 shape A/S), which uses confocal technology and enables integration with CAD software programs and CAM devices from other manufacturers.
CONE BEAM COMPUTED TOMOGRAPHY
CBCT is a technique that allows for 3D observation of structures related to the maxillofacial area. CBCT uses a round or rectangular cone-shaped x-ray beam, performing 180-360 degree rotations around the head of the patient. We can zoom through tissues to explore the gums, teeth and vital areas like sinuses. The clarity of the image allows us to measure the thickness of the bone and orientation of the nerves. It act as an implant surgical guides for oral surgeons and periodontists when placing dental implants, which in turn makes the treatment accurate than before. Thus it enables to place implants with greater precession and also to diagnose TMJ problems.6

Figure 2.1: A CBCT device integrated with cephalometric and panoramic radiographic functons (Cranex 3D, Soredex, Tuusula, Finland)
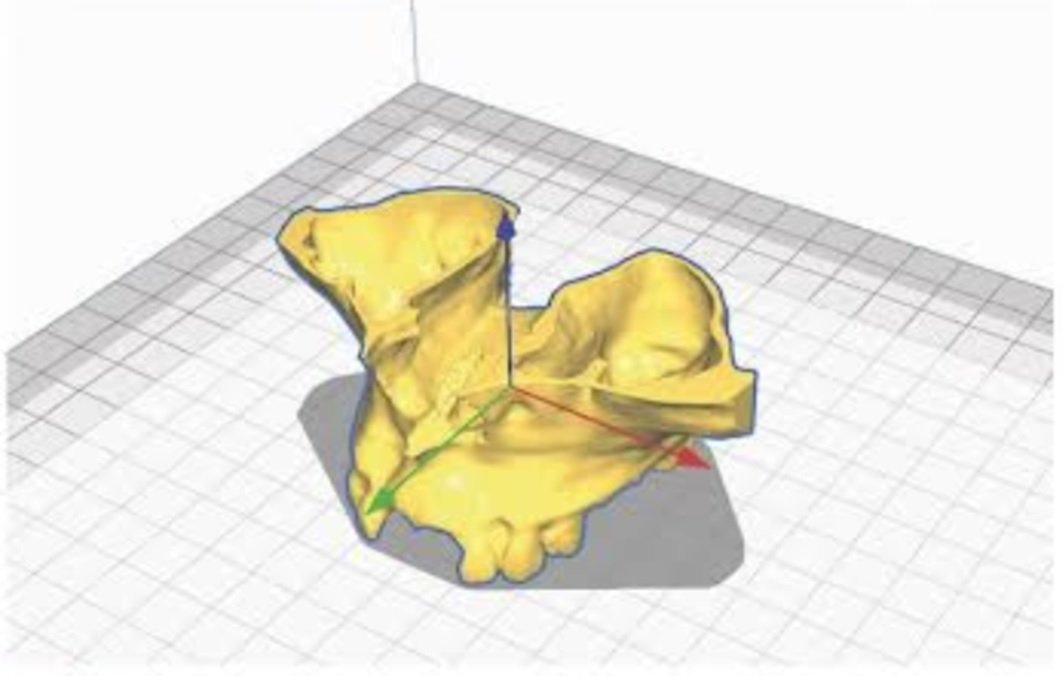
Figure: 2.2 A 3D object (reconstructed model of a maxillary CBCT scan) is positioned in the 3D space of a software (Ultimaker Cura) to be 3D printed. Note the three axes depicted by the software in different colors ( x-axis in red, y-axis in green, z-axis in blue).
CARIES DIAGNOSIS
Diagnodent is designed to aid in early detection of caries by measuring the increased light induced fluorescence. Visual examination and dental explorers help us to find decay on the surfaces of teeth and x-rays show us advanced decay and decay between the teeth. However, these methods don’t find decay that’s located inside the tooth. So these digital technologies help us to diagnose the hidden decay were the light probe scans the teeth with laser light. When laser reaches decay under the surface of the tooth, the decay emits the fluorescent light that bounces back to the sensors and it is translated into the digital read out and also as audible signal. Higher the value greater is the amount of decay in the tooth. The advanced technology uses sound, pulse and laser to detect caries earlier than the traditional methods. This in turn allows the dentist to commence the treatment immediately. With this advanced technology, we can more accurately and reliably find the decay in its earlier stages before it causes more damage and helps to preserve the healthy tooth structure.7.
DIGITAL PATIENT EDUCATION – PRACTICE AND PATIENT RECORD MANAGEMENT
The first and foremost frequent acquisition in the digital dentistry is the implementation of computers into each operatory as well as throughout the practice. 3 In most of the developed countries, this has reached the “early majority” stage while the dentists who have not yet acquired this prerequisite for digital dentistry should do so now. The advances and the improved software adapted from other industries allow this technology to be affordable and attain the fastest adoption rate as well as offer a high return on investment. The current highly effective systems include Dentrix, Practice Works, Eaglesoft and Webbased software like Curve Dental. The digital patient education is growing very rapidly.2,3 The future in this field will reveal the technologies as well as methods of communication which are already available in the other industries like touch-screen computer and/or voice-activated software instruction, rapid recall of photos and educational components, live video and 3-D video presentation with and without the tablets or monitors as well as off-site live consultation and education. However, there are many effective options for the digital patient education, such as CAESY, Guru, DDS GP for iPad, Consult-PRO Chairside, etc. A recent CR Foundation (clinicians report) has done a survey of more than 1,000 dentists which revealed that 80% would consider purchasing a tablet or an iPad or tablet for patients’ education.8
DIGITAL IMAGING/DIGITAL RADIOGRAPHY
Digital radiography is the latest advancement in dental imaging and is slowly being adopted by the dental profession. Digital imaging incorporates computer technology in the capture, display, enhancement and storage of direct radiographic images. Digital imaging offers some distinct advantages over film, but like any emerging technology, it presents new and different challenges for the practitioner to overcome. Today, dental offices have access to digital radiography. The advantages of using a sensor to capture data are immediate viewing, exposure time reduction and storage. The image can be transferred to other rooms such as Dentist Private Office for viewing or even emailed to specialists for consultation using a HIPAA-compliant email service. Images can be enlarged and enhanced to provide a comprehensive diagnosis and evaluation. Digital imaging uses up to 256 shades of grey compared with conventional film. There is 60% reduction in radiation exposure when using digital imaging. It also helps to reduce environmental impact bar film packets, which contains lead and processing solution is no longer used. These images can be stored and compared with previous or future images to estimate the dental health of the patient.9 The future improvements will use the algorithms based upon thousands of the patient radiographs that accurately diagnose the caries and also make the suggestions for dentist. Complete conversion to the extraoral imaging is the potential possibility for the future. Currently, there are many excellent intraoral digital radiography systems such as Kodak, Schick, Dexis, ScanX , Gendex etc.
IMPLANT TREATMENT PLANNING SOFTWARE
The dental implants has been one of the most important changes in the field of dentistry since 1983. Since then, treatment with dental implants has become one of the most predictable ways to replace lost teeth. There are many brands of implant systems to choose from today. The success of the implant is dependent on correct placement as well as several other factors such as Osseo-integration. Presurgical treatment planning software is designed to increase this efficiency of placing implants. Surgical templates assist in proper placement for esthetics restorative and functional purposes making implant placement faster, easier, safer and more precise. Thus, treatment planning, diagnosis, and placement of implant is easy and more accurate. Treatment planning software incorporates a digital scan either from an intraoral digital scanner or from a 3D image from a CBCT scan.10
Some implant companies have their own systems.11
- 3M True Definition • (3m.com/3M/en_US/Dental/)
- Carestream CS 3500 (carestreamdental.com)
- iTero by Align Technology (itero.com)
- The DWIO system from Dental Wings (dentalwings.com)
- PlanScan from Planmeca (planmecacadcam.com)
- Trios from 3Shape (www.3shape.com)
- CEREC (sirona.com)
- Lythos by Ormco (ormco.com)
DIODE LASER
Lasers are defined as monochromatic electromagnetic energy of one wavelength. Diode lasers are most commonly used soft tissue lasers by dentists. It is used for a variety of procedures such as soft-tissue gingivectomy, biopsy, impression toughing, frenectomy, adjunct periodontal procedures, implantlogy, in endodontic, and for tooth whitening. The infrared wavelengths of the laser have the ability to precisely and efficiently cut, coagulate, ablate, or vaporize the target tissue. Manufacturers have made the units small, portable, cordless, and low in cost, which make them desirable and easy to add the investment into the practice.12
Examples of dental laser companies include:
- Discus/Philips
- Ivoclar Vivadent
- Biolase
- AMD Lasers

Figure:2.2 Soft tissue dental lasers
DIGITAL WORKFLOW IN PERIODONTOLOGY
Nowadays, the concept of smile and dental esthetics is no longer limited to the teeth. The essential of a smile involve the relationship between the 3 components: the teeth, lip framework and the gingival scaffold. In spite of common notions about facial esthetics being usually based on subjective opinions and being influenced by cultural variants, emerging reaearch shows how the amount of gingival display significantly influences the perception of smile attractiveness, independent of age and sex. Excessive gingival display while smiling, also usually known as “ gummy smile” is a common esthetics concern among dental patients and being largely viewed as unesthetics, leads many patients to seek some form of treatment to address the issue.13
The planning of the surgical crown lengthening procedures has been broadly affected by the recent advent of the digital workflow in dentistry. CAD-CAM techniques have helped surgeons perform more precise and predictable surgeries, which contributes to fewer invasive procedures and better esthetic outcomes. Before digital guided surgery techniques, it was possible to use a vacuum-formed or acrylic resin surgical guide, made by diagnostic waxing to establish clinical crown length. The accuracy of these measurements varies according to the periodontal phenotype and site specific characteristics, including buccal bone thickness, gingival recession, root anatomy and tooth morphology.14
By integrating hard and soft tissue imaging data, obtained through IOS and CBCT methods, a 3D virtual patient can be created to noninvasively stimulate an entire treatment. This data integration, in turn, can predict digital workflow treatments.
By providing precise information and allowing 3D evaluation of the support periodontal tissues, CBCT acquisition is important not only for the diagnosis of the patients condition but also for precise and predictable periodontal planning. Clinical case and technique reports involving the manufacture of digital surgical guides to orient both the osteotomy and gingivectomy procedures during crown lengthening surgeries have used different computer programs to perform the periodontal profile analysis. This software evaluation allows for estimation of the ideal amount of tissue to be resected, by the assessment of the tomography to observe the relationship between biological distances and define the best surgical approach.
A surgical guide can be virtually modeled and 3-D printed to orient both incision and osteotomy related to the crown-lengthening surgical procedure.15
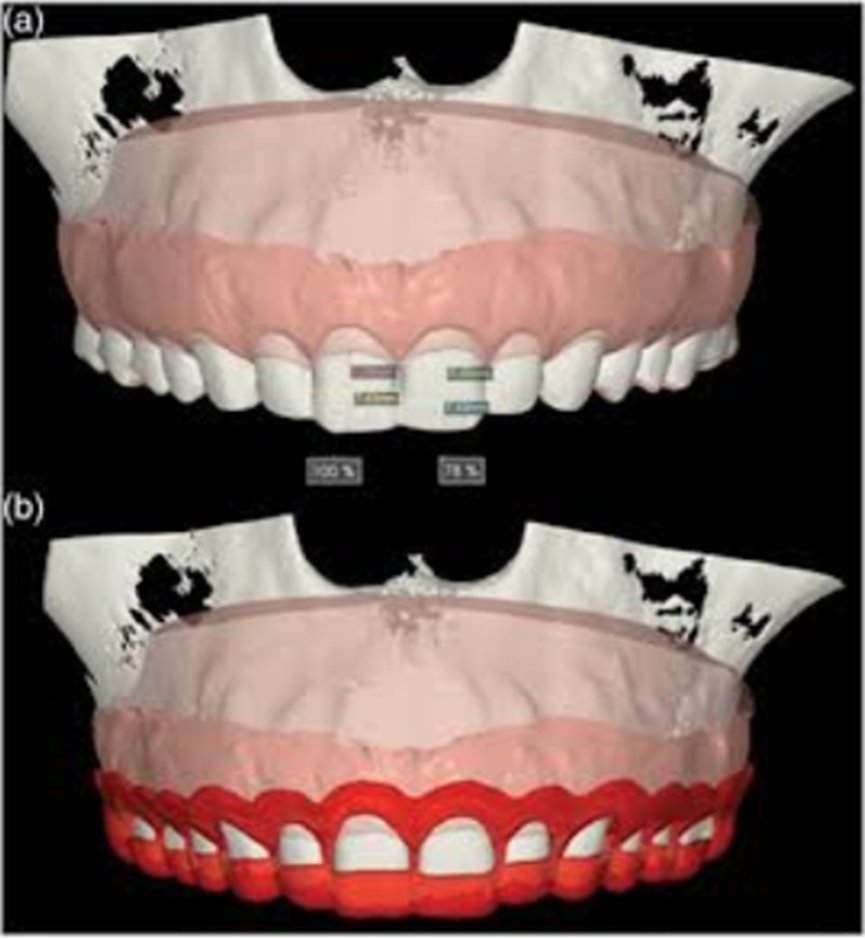
Figure:2.3 Periodontal surgical planning and guide design. The surgical guide is then impressed by a 3-D device using polymerizable resin ( thickness of 1.5mm). Following this the printed guide is washed in isopropyl alcohol for 15 minutes to remove unpolymerized resin residues on the surface, then it is

Figure:3.1 Using the periodontal guide for orienting internal bevel incisions on gingival margins.

Figure:3.2 Using the periodontal guide for bone recontour.
ADVANTAGES OF DIGITAL DENTISTRY
- Improved efficiency-Both cost and time.
- Less chair side time using digital technology.
- Improved accuracy in comparison to previous methods.
- High level of predictability of outcome.
- Technology will make practice management more efficient.
- Patient experience tends to be better and more comfortable when using digital treatments, with a sense of quality and a high level of technological innovation.
- Educational software and intelligent assistants will increasingly support the needs for decision making in clinical practice.16

Figure 4.1: Digital workflow involving imaging and planning centers. All treatment plans are ultimately to be approved by the dental clinician responsible for the case.
LIMITATIONS OF DIGITAL DENTISTRY
- The major limitation of most areas of digital dentistry is cost. To adopt new technology often requires a higher capital investment, especially at the “innovator” or “early adopter” stage.
- The other main limitation for the clinician to explore these new advancing dental technology is lack of training, knowledge and desire.
- Misunderstanding the new technology tends to faster slower adoption rates.17
CONCLUSION
Digital dentistry has transformed the field of dentistry, improving the precision, accuracy and efficiency of dental procedures, as well as patient outcomes. Digital dentistry has revolutionized the way dental professionals provide patient care, allowing for greater precision, efficiency and accessibility. Advancements in imaging, CAD/CAM technology, 3D printing, and regenerative dentistry have transformed the dental industry. Going completely digital is the right decision. There is no doubt in mind that this is the future of dentistry and future of dental education, the future of oral care. When properly implemented and fully educated, return on investment can be excellent, increased joy in practicing dentistry can be experienced, and better care for patients can be delivered.
ACKNOWLEDGEMENT:
The authors wish to express their sincere gratitude to Professor, Department of Periodontology and Oral Implantology, Kanti Devi Dental College and Hospital, Atal Bihari Vajpayee Medical University, Lucknow, India for providing necessary facilities to carry out this review work.
REFERENCES
- Paul L. Child J R, Jr, DMD, CDT, CEO. Digital dentistry: Is this the future of dentistry?, CR Foundation, www.dentaleconomics.com.
- Ireland R S, Jenner A M, Williams M J, Tickle M. A clinical minimum data set for primary dental care. Br Dent J 2017; 190: 663-667.
- Burke F J, Busby M, McHugh S, Delargy S, Mullins A, Matthews R. Evaluation of an oral health scoring system by dentists in general dental practice. Br Dent J 2013; 194: 215-218.
- Sjogren G, Molin M, Van Dijken JW. A 10- year prospective evaluation of CAD/CAM manufactured (Cerec) ceramic inlays cemented with a chemically cured or dual- cured resin composite, Int J Prosthodont, 17(2), 2004, 241- 46.
- Talwar S, Utneja S, Nawal RR, Kaushik A, Srivastava D, Oberoy SS. Role of Cone- beam Computed Tomography in Diagnosis of Vertical Root Fractures: A Systematic Review and Metaanalysis, J Endod, 42(1), 2016, 12
- Dental Practice Board. Dental computer survey. London: Department of Health NHS Management Executive, 2017
- D. Rekow (Ed.), Digital dentistry: a comprehensive reference and preview of the future, Quintessence, Berlin (2018), pp. 19-40
- Baumgarten HS, Wunsche A. CAD/CAM Fabrication of Definitive Implant Prostheses: A Digital Workflow Planning to Implant Placement to Final Restoration, Compend Contin Educ Dent, 36(10), 2015, 746-55.
- Davidowitz, G and kotick, PG. (2011). The use of CAD/CAM in dentistry. Dent. Clin. North Am. 55 (3):559-570.
- Bagis, N, Kolsuz, M.E, Kursun S., and Orban, K. (2015). Comparison of intraoral radiography and cone-beam computed tomography for the detection of periodontal defects: an invitro study. BMC Oral Health 15:64.
- Nasseh,I. and AL-Rawi, W. (2018). Cone beam computed tomography. Dent.Clin. North Am. 62 (3): 559-570.
- Coachman, C, Sesma, N., and Blatz, M.B. (2021). The complete digital workflow in interdisciplinary dentistry. Int. J., Esthet. Dent. 16: 1-18.
- Rizzante FA, Maenosono RM, Duarte MA, Furuse AY, Palma-Dibb R G, Ishikiriama SK. In Vitro Evaluation of Dentin Hydraulic Conductance after 980 Nm Diode Laser Irradiation, J Periodontol, 87(3), 2016, 320- 6.
- Romero L, Jiménez M, Espinosa Mdel M, Dominguez M. New Design for Rapid Prototyping of Digital Master Casts for Multiple Dental Implant Restorations, PLoS One, 11(2), 2015, 10.
- Kurt Bayrakdar, S. Orhan, K., Bayrakdar, I.S. et al. (2021). A deep learning approach for dental implant planning in cone- beam computed tomography images. BMC Med. Imaging 21 (1): 86.
- Garber, D.A and Salama, M.A. (1996). The esthetic smile: diagnosis and treatment. Periodontology 2000. (11): 18-28.
- Kaya, B and Uyar, R. (2013). Influence on smile attractiveness of the smile arc in conjunction with gingival display. Am J . Orthod. Dentofacial Orthop. 144 (4): 541-547.
- Liu, X., Yu, J., Zhou, J., and Tan, J. (2018). A digitally guided dual technique for both gingival and bone resection during crown lengthening surgery.J. Prosthet. Dent. 119 (3): 345-349.
- Passos, L., Soares, F.P., Choi, I.G.G., and Cortes, A.R.G. (2020). Full digital workflow for crown lengthening by using a single surgical guide.J. Prosthet. Dent. 124 (3): 257-261.