ABSTRACT
This case report presents a patient who had been rehabilitated with implants supported maxillary and mandibular screw retained PFM prosthesis. Five implants were successfully placed in each maxillary and mandibular arch and no complications occurred in the postoperative or maintenance periods. Four months after the prosthesis was delivered; which was found to be clinically, biologically, and mechanically stable, and the patient was satis?ed with the esthetics and her ability to function.
INTRODUCTION
Complete oral rehabilitation is always very demanding and requires careful planning of the course of treatment. Individuals may experience early tooth loss as a result of periodontal issues and severe dental caries.1 Prosthetic rehabilitation of partial edentulism can be done with plenty of contemporary and conventional treatment modalities. Implant-supported prostheses have become widely preferred prosthetic approach and treatment choice because of their reliable functional and aesthetic results.2
In addition to implant therapy, achieving a patient's high aesthetic standards requires achieving a number of biological and mechanical objectives. Fixed dental prosthesis (FDPs) and porcelain veneered single crowns are well renowned for their wear resistance, colour stability, biocompatibility, and pleasing aesthetics.3
CLINICAL REPORT
A 75 year old male patient reported to the department of Prosthodontics with a chief complaint of inability to chew because of missing teeth. After obtaining his medical and dental history, he was examined clinically and radiographically. It was found that he had lost many of the teeth in the maxillary and Mandibular arch due to periodontal diseases and decay. Pre operative inta oral photographs were taken. (Fig. 1 and Fig. 2)
Intraoral examination revealed absence of 12,13,15,16,24,25,26,27,31,32,33,34,35,36,37,41,45,46,47.

Fig. 1: Pre-operative Maxilla

Fig. 2: Pre operative mandible
The OPG( Fig .3) was taken to evaluate the condition of the teeth that were present and the condition of the bone for implants. Patient was well informed and explained about the various treatment options like removable and implant supported fixed prostheses.

Fig .3: PREOPERATIVE INTRAORAL RADIOGRAPH
Considering the remaining teeth, periodontal tissues health and patient expectations/benefits, it was decided to rehabilitate with implant supported maxillary and mandibular fixed partial denture.
An open-flap surgery was performed and genesis dental implants were placed in the region of incisor, canine, first premolar and first molar
After 4 months of osseointegration of implants, second stage surgery was performed and healing abutments were placed(Fig. 4 – a & b).


Fig. 4 (a&b): AFTER SECOND STAGE SULCUS FORMER PLACED
Two weeks later, impression coping were placed, splinted together intraorally with dental floss and an open tray impression (Fig. 5) was made using cold cure acrylic resin customized tray.

Fig. 5: OPEN TRAY IMPRESSION
The metal framework were tried in and checked for passivity of framework. Unglazed trail was done (Fig. 6 – a, b & c) Maxillary and Mandibular prosthesis with porcelain was delivered(Fig. 7 & Fig. 8).



Fig. 6 (a, b & c ): UNGLAZED TRIAL WAS DONE.



Fig. 7 (a, b & c ): POSTOPERATIVE INTRA ORAL VIEW

Fig. 8: PROSTHESIS DELIVERED
All the prosthetic screws were given an end most torque of 15N/cm.4 The prosthetic screw access holes were sealed with composite material. The occlusion was evaluated and adjusted to a mutually protected occlusion scheme keeping in mind the patient's centric relation.
The patient was recalled for follow up visits every 6 weeks during the first 3 months, 6 months after the insertion of de?nitive prostheses. At 6 months, the prosthesis was removed and biological and mechanical complications were assessed. Further follow-ups visits were carried out at 12 and 18 months after delivery of the prosthesis(Fig. 9).
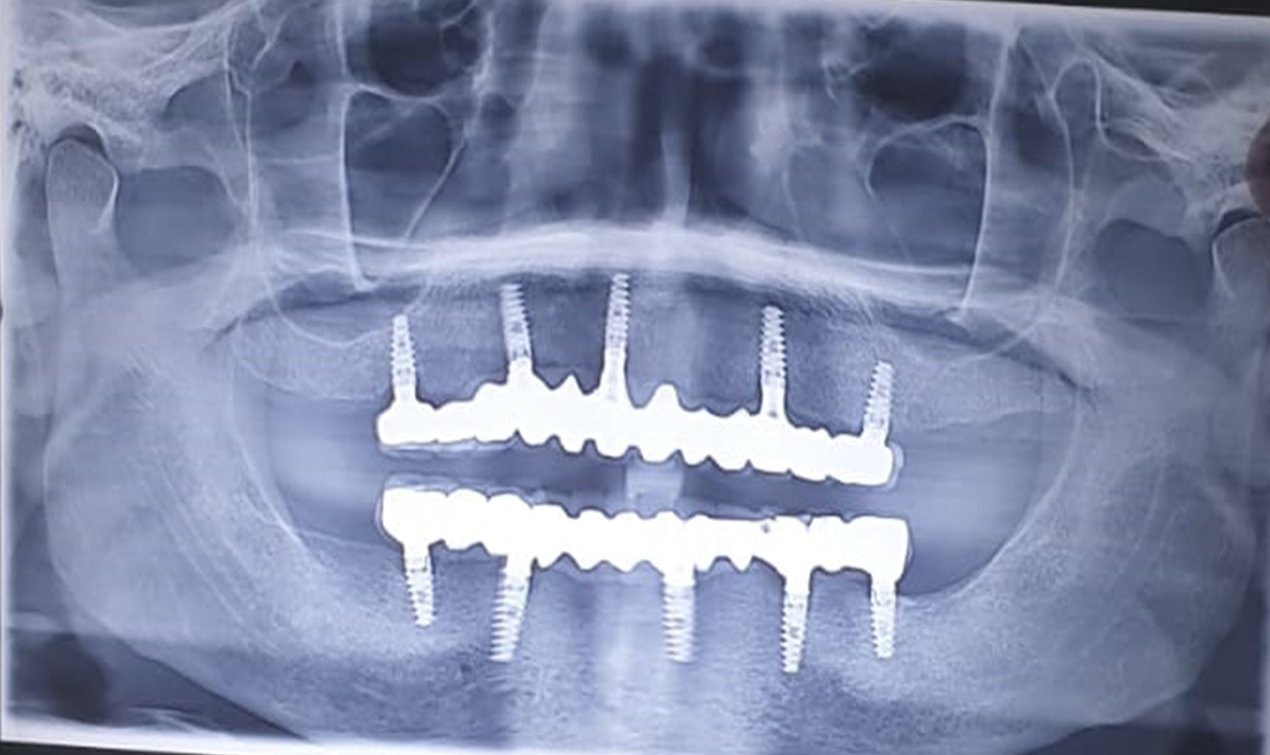
Fig. 9: 18 MONTH FOLLOW UP
DISCUSSION
Proper diagnosis and precise treatment planning are key to success for implant rehabilitation. Implant-supported FPD is a viable treatment option in the literature and has shown predictable long-term outcome.
In the current case report, fixed full-arch implant rehabilitation was selected for the definitive prosthetic design of the maxillary and mandibular arch. The distribution of implants was followed according to the prosthodontic plan. The maxillary and mandibular arch included a five-unit implant supported PFM.
CONCLUSION
An excellent prognosis can be given for the present treatment, assuming continued favorable patient compliance with regard to oral hygiene maintenance. Implant supported fixed partial denture is a good alternative to the conventional complete dentures due to the better reconstruction of the patient's functional, phonation, and esthetic requirements.
REFERENCES
- Maló P, de Sousa ST, De Araújo Nobre M, Moura Guedes C, Almeida R, Roma Torres A, Legatheaux J, Silva A. Individual Lithium Disilicate Crowns in a Full-Arch, ImplantSupported Rehabilitation: A Clinical Report. J Prosthodont 2014 Aug; 23(6):495-500.
- Dede DÖ, Cenk Durmuslar M, Sah?n O, Koroglu A, Is?sag O. Telescopic Overdenture and Implant Supported Fixed Partial Denture: A Pragmatic Treatment Approach. Case Rep Dent 2015; 1-7.
- Maló P, de Sousa ST, De Araújo Nobre M, Moura Guedes C, Almeida R et al. A Individual Lithium Disilicate Crowns in a Full-Arch, Implant-Supported Rehabilitation: A Clinical Report. J Prosthodont 2014 Aug; 23(6):495500.
- Traini T, Mangano C, Sammons RL, Mangano F, Macchi A, Piattelli A. Direct laser metal sintering as a new approach t o fabrication of an isoelastic functionally graded material for manufacture of porous titanium dental implants. Dent Mater. 2008; 24:1525-33.
- Quante K, Ludwig K, Kern M. Marginal and internal fit of metal-ceramic crowns fabricated with a new laser melting technology. Dent Mater. 2008; 24:1311-5.
- Bhaskaran E, Azhagarasan NS, Miglani S, Ilango T, Krishna GP, Gajapathi B. Comparative evaluation of marginal and internal gap of Co-Cr copings fabricated from conventional wax pattern, 3D printed resin pattern and DMLS tech: An in vitro study. J Indian Prosthodont Soc. 2013; 13:189-95.